
Use of LILETTA is contraindicated in women with the following: pregnancy; for use as post-coital contraception; congenital or acquired uterine anomaly, including leiomyomas, that distorts the uterine cavity and would be incompatible with correct intrauterine system (IUS) placement; known or suspected breast cancer or other...
Use of LILETTA is contraindicated in women with the following: pregnancy; for use as post-coital contraception; congenital or acquired uterine anomaly, including leiomyomas, that distorts the uterine cavity and would be incompatible with correct intrauterine system (IUS) placement; known or suspected breast cancer or other hormone-sensitive cancer, now or in the past; known or suspected uterine or cervical malignancy; acute liver disease or liver tumor; untreated acute cervicitis or vaginitis, including lower genital tract infections (eg, bacterial vaginosis), until infection is controlled; postpartum endometritis or infected abortion in the past 3 months; unexplained uterine bleeding; a current IUS; acute pelvic inflammatory disease (PID); conditions increasing susceptibility to pelvic infection; or hypersensitivity to any component of LILETTA.
Use LILETTA with caution after careful assessment in women with coagulopathy or taking anticoagulants; migraine, focal migraine with asymmetrical visual loss, or other symptoms indicating transient cerebral ischemia; exceptionally severe or frequent headache; marked increase of blood pressure; or severe arterial disease such as stroke or myocardial infarction. Consider removing LILETTA if the following arise during use: uterine or cervical malignancy or jaundice. Because irregular bleeding/spotting is common during the first months of LILETTA use, exclude endometrial pathology (polyps or cancer) prior to the insertion of LILETTA in women with persistent or uncharacteristic bleeding. If the threads are not visible or are significantly shortened, they may have broken or retracted into the cervical canal or uterus. If LILETTA is displaced (eg, expulsed or perforated the uterus), remove it.
If pregnancy should occur with LILETTA in place, remove the IUS because leaving it in place may increase the risk of spontaneous abortion and preterm labor. Removal or manipulation may result in pregnancy loss. Evaluate women for ectopic pregnancy because the likelihood of a pregnancy being ectopic is increased. Tell women about the signs of ectopic pregnancy and associated risks, including loss of fertility. Women with a history of ectopic pregnancy, tubal surgery, or pelvic infection have a higher risk of ectopic pregnancy.
Insertion of LILETTA is contraindicated in the presence of known or suspected PID or endometritis. IUSs have been associated with an increased risk of PID, most likely due to organisms being introduced into the uterus during insertion. In the LILETTA contraception study, one woman diagnosed with PID and two women diagnosed with endometritis developed the infection within a week of insertion. One endometritis case was diagnosed at 39 days after insertion. The remaining 11 cases of PID and endometritis were diagnosed more than 6 months after insertion, including one at 30 days after IUS removal. In the HMB study, one woman was diagnosed with PID about 5 months after LILETTA insertion. Counsel women who use LILETTA to notify a healthcare provider if they develop lower abdominal or pelvic pain, fever, chills, unusual or malodorous discharge, unexplained bleeding, genital lesions or sores, or dyspareunia. PID and endometritis are often associated with sexually transmitted infections (STIs); LILETTA does not protect against STIs, including HIV. PID or endometritis may be asymptomatic but still result in tubal damage and its sequelae. Inform women about the possibility of PID or endometritis and that these infections can cause tubal damage leading to ectopic pregnancy or infertility, or infrequently can necessitate hysterectomy, or cause death.
Spotting and irregular or heavy bleeding may occur during the first 3 to 6 months. Periods may become shorter and/or lighter thereafter. Cycles may remain irregular, become infrequent, or even cease. Consider pregnancy, including ectopic pregnancy, if menstruation does not occur within 6 weeks of the onset of previous menstruation. If a significant change in bleeding develops during prolonged use, conduct diagnostic tests to assess possible endometrial pathology.
Some serious complications with IUSs like LILETTA are sepsis, perforation, and expulsion. Severe infection or sepsis, including Group A streptococcal sepsis (GAS), have been reported following insertion of LNG-releasing IUSs. Aseptic technique during insertion of LILETTA is essential to minimize serious infections such as GAS.
Perforation (total or partial, including penetration/embedment of LILETTA in the uterine wall or cervix) may occur, most often during insertion, although the perforation may not be detected until sometime later. Perforation may also occur at any time during use. Perforation may reduce contraceptive efficacy. If perforation is suspected, locate and remove LILETTA as soon as possible. Surgery may be required. Delayed detection or removal of LILETTA in case of perforation may result in migration outside the uterine cavity, adhesions, peritonitis, intestinal perforations, intestinal obstruction, abscesses, and erosion of adjacent viscera. The risk of perforation is increased if inserted in women who have fixed retroverted uteri, are postpartum, or are lactating. Delay LILETTA insertion a minimum of 4 weeks or until uterine involution is complete following a delivery or a second-trimester abortion.
Partial or complete expulsion of LILETTA may occur, resulting in the loss of contraceptive protection. Expulsion risk is increased when inserted immediately after delivery; it appears to be increased with insertions after second-trimester abortion, based on limited data. Risk of expulsion is increased for patients with a history of HMB or greater than normal BMI at the time of insertion. Remove a partially expelled LILETTA. If expulsion has occurred, a new LILETTA may be inserted when there is reasonable certainty the patient is not pregnant.
Ovarian cysts may occur and are generally asymptomatic. Cysts may be accompanied by pelvic or abdominal pain or dyspareunia. Evaluate persistent ovarian cysts.
In the LILETTA contraception study, the most common adverse reactions (≥5% users) were vulvovaginal mycotic infections (20.2%), vaginal bacterial infections (19.2%), acne (15.5%), nausea or vomiting (10.5%), headache (10.1%), breast tenderness or pain (10.1%), abdominal discomfort or pain (10.0%), dyspareunia (9.6%), anxiety (9.6%), depression (9.1%), pelvic discomfort or pain (8.7%), dysmenorrhea (7.3%), mood changes (6.5%), back pain (6.5%), increased weight (6.1%), and vaginal discharge (5.8%). In the LILETTA HMB study, the adverse reaction profile was consistent with the adverse reaction profile in the contraception study.
Teach patients to recognize and immediately report signs or symptoms of the aforementioned conditions. Consider evaluating patients 4 to 6 weeks after LILETTA insertion and during routine care, or more often if clinically indicated. Check threads during each evaluation.
Please see full Prescribing Information.
THE LILETTA® ACCESS IUS TRIAL:*†
THE LARGEST HORMONAL IUD
STUDY CONDUCTED EXCLUSIVELY
IN U.S. WOMEN1
In nulliparous and parous women aged 16 to 45 years across a wide range of BMIs (15.8 kg/m2 to 61.6 kg/m2)1


EVALUATED OVER THE COURSE OF 8 YEARS1
Open-label, multicenter trial conducted at 30 U.S. study centers over 96 months

PRIMARY OUTCOME1
Efficacy of LILETTA for pregnancy prevention in women of childbearing potential

SECONDARY OUTCOMES2
- Safety and bleeding patterns
- Return of menses after discontinuation
- Pregnancy rates after discontinuation
BMI=body mass index.
*LILETTA is an intrauterine system, or IUS, otherwise known as an IUD, intrauterine device.
†ACCESS IUS=A Comprehensive Contraceptive Efficacy and Safety Study of an IUS.2
BMI=body mass index.
*LILETTA is an intrauterine system, or IUS, otherwise known as an IUD, intrauterine device.
†ACCESS IUS=A Comprehensive Contraceptive Efficacy and Safety Study of an IUS.5
STUDY POPULATION: A STUDY THAT INCLUDED A DIVERSE GROUP OF U.S. WOMEN1
The ACCESS IUS trial studied LILETTA in 1751 generally healthy patients.
 Parity1
Parity1
nulliparous women
parous women

 BODY MASS INDEX (BMI)1
BODY MASS INDEX (BMI)1
Overall range
Mean BMI
 AGE1
AGE1
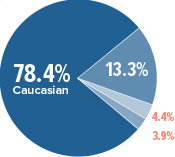
 RACE AND ETHNICITY1
RACE AND ETHNICITY1
Caucasian
Black/
African American
Other
of women indicated Hispanic ethnicity.
EFFICACY SHE WANTS, WITHOUT DAILY MAINTENANCE,‡ DEMONSTRATED FOR UP TO 8 YEARS1
Effective, long-acting, reversible contraception for up to 8 years1
year 1
over 8 years
Primary endpoint was the pregnancy rate calculated as the Pearl Index in women aged 16-35 (Years 1-6) and aged 16-39 (Years 7-8).
‡Patients should be counseled to check that LILETTA is in the proper position by feeling the threads once a month. After placement, healthcare providers should consider re-examining patients 4 to 6 weeks after insertion and during routine care, or more often if clinically indicated. Check threads during each evaluation.
REVERSIBILITY: A LONG-ACTING, REVERSIBLE CONTRACEPTIVE METHOD FOR UP TO 8 YEARS1
DISCONTINUATION OF LILETTA1
Data based on an analysis of 244 women who desired pregnancy after study discontinuation.
Conception rates after removal of LILETTA were assessed and appeared consistent with conception rates in the general population of women having regular, unprotected sexual intercourse for 12 months.
LILETTA® is a sterile, levonorgestrel-releasing intrauterine system indicated for prevention of pregnancy for up to 8 years; replace after 8 years if continued use is desired. LILETTA is indicated for the treatment of heavy menstrual bleeding (HMB) for up to 5 years in women who choose intrauterine contraception as their method of contraception; replace after 5 years if continued HMB treatment is needed.
Use of LILETTA is contraindicated in women with the following: pregnancy; for use as post-coital contraception; congenital or acquired uterine anomaly, including leiomyomas, that distorts the uterine cavity and would be incompatible with correct intrauterine system (IUS) placement; known or suspected breast cancer or other hormone-sensitive cancer, now or in the past; known or suspected uterine or cervical malignancy; acute liver disease or liver tumor; untreated acute cervicitis or vaginitis, including lower genital tract infections (eg, bacterial vaginosis), until infection is controlled; postpartum endometritis or infected abortion in the past 3 months; unexplained uterine bleeding; a current IUS; acute pelvic inflammatory disease (PID); conditions increasing susceptibility to pelvic infection; or hypersensitivity to any component of LILETTA.
Use LILETTA with caution after careful assessment in women with coagulopathy or taking anticoagulants; migraine, focal migraine with asymmetrical visual loss, or other symptoms indicating transient cerebral ischemia; exceptionally severe or frequent headache; marked increase of blood pressure; or severe arterial disease such as stroke or myocardial infarction. Consider removing LILETTA if the following arise during use: uterine or cervical malignancy or jaundice. Because irregular bleeding/spotting is common during the first months of LILETTA use, exclude endometrial pathology (polyps or cancer) prior to the insertion of LILETTA in women with persistent or uncharacteristic bleeding. If the threads are not visible or are significantly shortened, they may have broken or retracted into the cervical canal or uterus. If LILETTA is displaced (eg, expulsed or perforated the uterus), remove it.
If pregnancy should occur with LILETTA in place, remove the IUS because leaving it in place may increase the risk of spontaneous abortion and preterm labor. Removal or manipulation may result in pregnancy loss. Evaluate women for ectopic pregnancy because the likelihood of a pregnancy being ectopic is increased. Tell women about the signs of ectopic pregnancy and associated risks, including loss of fertility. Women with a history of ectopic pregnancy, tubal surgery, or pelvic infection have a higher risk of ectopic pregnancy.
Insertion of LILETTA is contraindicated in the presence of known or suspected PID or endometritis. IUSs have been associated with an increased risk of PID, most likely due to organisms being introduced into the uterus during insertion. In the LILETTA contraception study, one woman diagnosed with PID and two women diagnosed with endometritis developed the infection within a week of insertion. One endometritis case was diagnosed at 39 days after insertion. The remaining 11 cases of PID and endometritis were diagnosed more than 6 months after insertion, including one at 30 days after IUS removal. In the HMB study, one woman was diagnosed with PID about 5 months after LILETTA insertion. Counsel women who use LILETTA to notify a healthcare provider if they develop lower abdominal or pelvic pain, fever, chills, unusual or malodorous discharge, unexplained bleeding, genital lesions or sores, or dyspareunia. PID and endometritis are often associated with sexually transmitted infections (STIs); LILETTA does not protect against STIs, including HIV. PID or endometritis may be asymptomatic but still result in tubal damage and its sequelae. Inform women about the possibility of PID or endometritis and that these infections can cause tubal damage leading to ectopic pregnancy or infertility, or infrequently can necessitate hysterectomy, or cause death.
Spotting and irregular or heavy bleeding may occur during the first 3 to 6 months. Periods may become shorter and/or lighter thereafter. Cycles may remain irregular, become infrequent, or even cease. Consider pregnancy, including ectopic pregnancy, if menstruation does not occur within 6 weeks of the onset of previous menstruation. If a significant change in bleeding develops during prolonged use, conduct diagnostic tests to assess possible endometrial pathology.
Some serious complications with IUSs like LILETTA are sepsis, perforation, and expulsion. Severe infection or sepsis, including Group A streptococcal sepsis (GAS), have been reported following insertion of LNG-releasing IUSs. Aseptic technique during insertion of LILETTA is essential to minimize serious infections such as GAS.
Perforation (total or partial, including penetration/embedment of LILETTA in the uterine wall or cervix) may occur, most often during insertion, although the perforation may not be detected until sometime later. Perforation may also occur at any time during use. Perforation may reduce contraceptive efficacy. If perforation is suspected, locate and remove LILETTA as soon as possible. Surgery may be required. Delayed detection or removal of LILETTA in case of perforation may result in migration outside the uterine cavity, adhesions, peritonitis, intestinal perforations, intestinal obstruction, abscesses, and erosion of adjacent viscera. The risk of perforation is increased if inserted in women who have fixed retroverted uteri, are postpartum, or are lactating. Delay LILETTA insertion a minimum of 4 weeks or until uterine involution is complete following a delivery or a second-trimester abortion.
Partial or complete expulsion of LILETTA may occur, resulting in the loss of contraceptive protection. Expulsion risk is increased when inserted immediately after delivery; it appears to be increased with insertions after second-trimester abortion, based on limited data. Risk of expulsion is increased for patients with a history of HMB or greater than normal BMI at the time of insertion. Remove a partially expelled LILETTA. If expulsion has occurred, a new LILETTA may be inserted when there is reasonable certainty the patient is not pregnant.
Ovarian cysts may occur and are generally asymptomatic. Cysts may be accompanied by pelvic or abdominal pain or dyspareunia. Evaluate persistent ovarian cysts.
In the LILETTA contraception study, the most common adverse reactions (≥5% users) were vulvovaginal mycotic infections (20.2%), vaginal bacterial infections (19.2%), acne (15.5%), nausea or vomiting (10.5%), headache (10.1%), breast tenderness or pain (10.1%), abdominal discomfort or pain (10.0%), dyspareunia (9.6%), anxiety (9.6%), depression (9.1%), pelvic discomfort or pain (8.7%), dysmenorrhea (7.3%), mood changes (6.5%), back pain (6.5%), increased weight (6.1%), and vaginal discharge (5.8%). In the LILETTA HMB study, the adverse reaction profile was consistent with the adverse reaction profile in the contraception study.
Teach patients to recognize and immediately report signs or symptoms of the aforementioned conditions. Consider evaluating patients 4 to 6 weeks after LILETTA insertion and during routine care, or more often if clinically indicated. Check threads during each evaluation.
Please see full Prescribing Information
References: 1. LILETTA (levonorgestrel-releasing intrauterine system) 52 mg [prescribing information]. North Chicago, IL: AbbVie Inc., and San Francisco, CA: Medicines360. 2. Data on file. ABVRRTI75507. 3. Data on file. ABVRRTI75116.